





Authors: Jens Neumann, João Aguiar Machado, Miriam Görtzen, Lena Geier
The global obesity treatment market is expanding at an unprecedented pace, with sales of weight loss medications forecast to rise dramatically over the next decade.1 GLP-1-based injectables such as Wegovy and Zepbound have redefined expectations for efficacy in weight loss, cardiovascular safety and metabolic benefits, stimulating sustained double-digit growth.1
At the same time, competition is intensifying. A growing array of treatment modalities and new entrants are crowding the market, with biotech companies promoting next-generation GLP-1 candidates alongside established pharmaceutical players. With more than 100 active GLP-1 clinical programmes worldwide, the bar for differentiation is rising rapidly.1 In parallel, semaglutide will become generic in some key markets from 2026 onward (e.g., India, China, Brazil), and pressure from compounding pharmacies to meet unmet demand for GLP‑1 therapies adds another layer of complexity and competition to the evolving treatment landscape.2,3
Against this backdrop, oral GLP-1 receptor agonists are emerging as an increasingly important area of focus, as companies look to extend growth beyond injectables and broaden access to obesity care.
Launch timeline of weight loss medication
Expected indication launch timelines for selected pipeline candidates
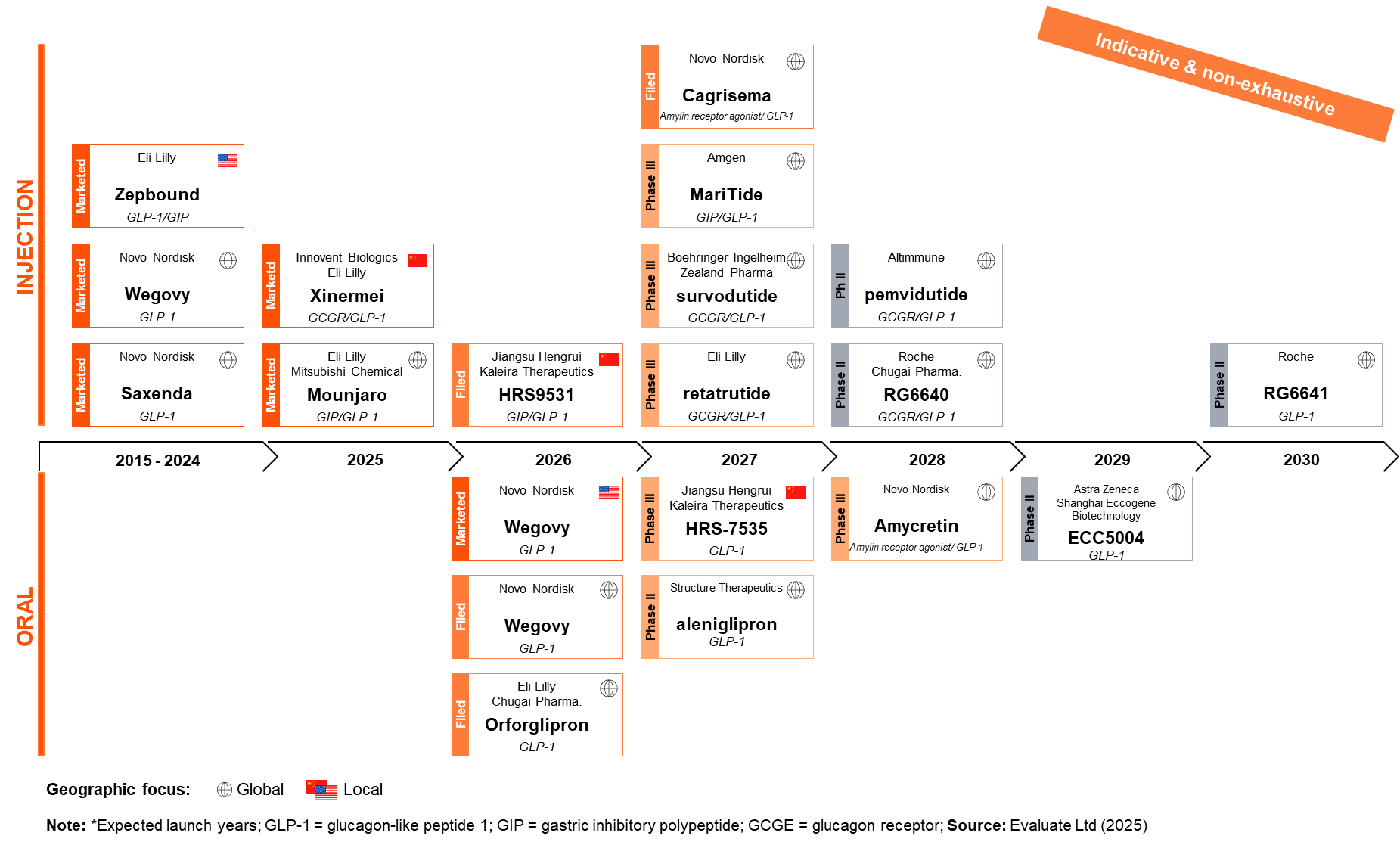
Pharmaceutical companies are investing significantly in oral GLP-1s. Recent moves underscore the scale of their commitment: Novo Nordisk’s oral semaglutide is now FDA-approved and available for obesity treatment in the US.4
These investments are being echoed across the manufacturing ecosystem. CDMOs are expanding oral solid dosage (OSD) capabilities to support anticipated demand.5 While oral delivery already dominates the pharmaceutical landscape – accounting for roughly 84% of top-selling medicines6– GLP-1s introduce greater complexity. As biologics, they require advanced manufacturing technologies, prompting targeted capital investments beyond conventional OSD infrastructure.
Combined, these developments offer a substantial opportunity to reshape the obesity market – expanding access, normalising long-term treatment and supporting large-scale adoption.
Why invest in oral GLP-1s in obesity?
Oral GLP-1s represent more than a change in dosage form; they signal a structural shift in how obesity can be treated, prescribed and scaled. Patient preference data – showing a strong bias towards oral therapies over injections7,8– points to a broader redefinition of engagement, adherence and long-term management. By removing the psychological and practical barriers associated with injectable treatments, oral GLP-1s have the potential to reposition obesity care as a routine, chronic intervention rather than a specialist-led, escalation therapy.
This shift enlarges the addressable market significantly. Oral formulations might enable obesity treatment to move decisively into primary care, extending its reach well beyond today’s specialist base and giving access to greater numbers of patients earlier in the course of the disease. In doing so, oral formulations could support the normalisation of obesity management – making initiation simpler for general practitioners and reducing the stigma that continues to limit the uptake of injectable therapies.9
At system level, oral GLP-1s also align with scalable healthcare delivery models. Their compatibility with established pharmaceutical supply chains – without the constraints of cold-chain logistics, injection training or medical-waste handling – creates opportunities to broaden distribution through retail pharmacies and remote care pathways. Collectively, these dynamics position oral GLP-1s as a catalyst for large-scale adoption, supporting access, acceptance and operational scalability in ways injectables cannot fully achieve.
Beyond obesity, the emergence of effective oral GLP-1s also highlights opportunities for a broader platform. Advances in peptide formulation, stabilisation and delivery that enable oral GLP-1s could be leveraged for other biologic therapies, opening new pathways for oral delivery in other conditions. As such, investments in oral GLP-1s may generate value well beyond a single indication, laying the groundwork for a new generation of orally delivered biologics.
Yet realising this promising potential will depend on overcoming manufacturing and commercial challenges that are far from trivial.
What are manufacturing and commercial challenges for oral GLP-1s in obesity?
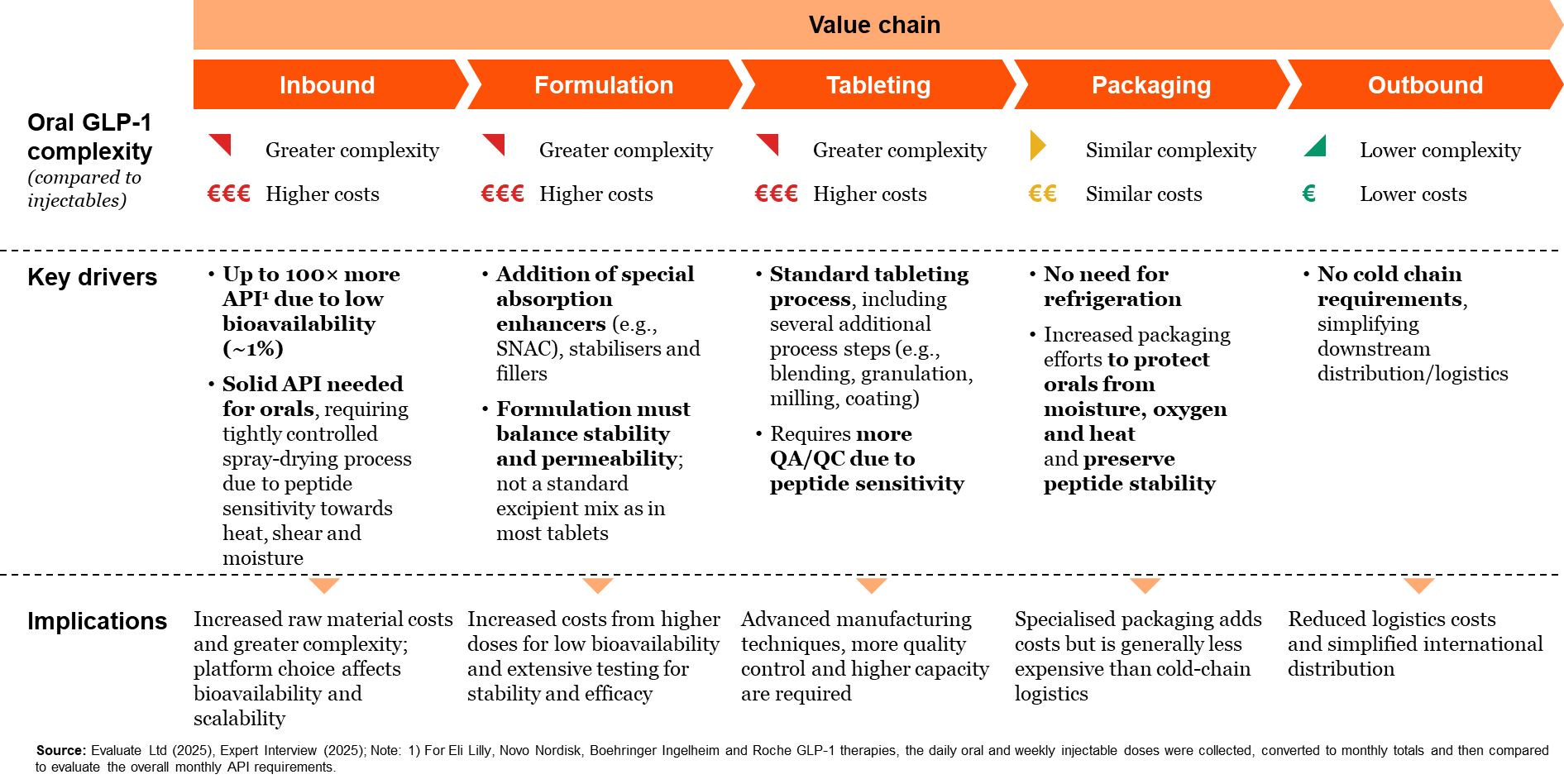
Oral GLP-1s simplify distribution and patient access but cause significantly greater complexity upstream in the value chain, creating a distinct set of operational challenges. Low oral bioavailability results in substantially higher API volume requirements, increasing raw material consumption and production intensity. Formulation requires specialised excipients and precise control to balance peptide stability, permeability and manufacturability. Although delivered as conventional tablets, oral GLP-1s require modified tableting processes, tighter environmental controls and enhanced quality oversight due to peptide sensitivity. Packaging must protect against moisture, oxygen and heat to preserve stability, despite eliminating cold-chain requirements. Collectively, these factors contribute to the currently higher costs of goods compared to injectable GLP-1s, reflecting additional material, process and quality complexity along the upstream value chain.
Complexity of oral vs. injectable GLP-1 value chain today
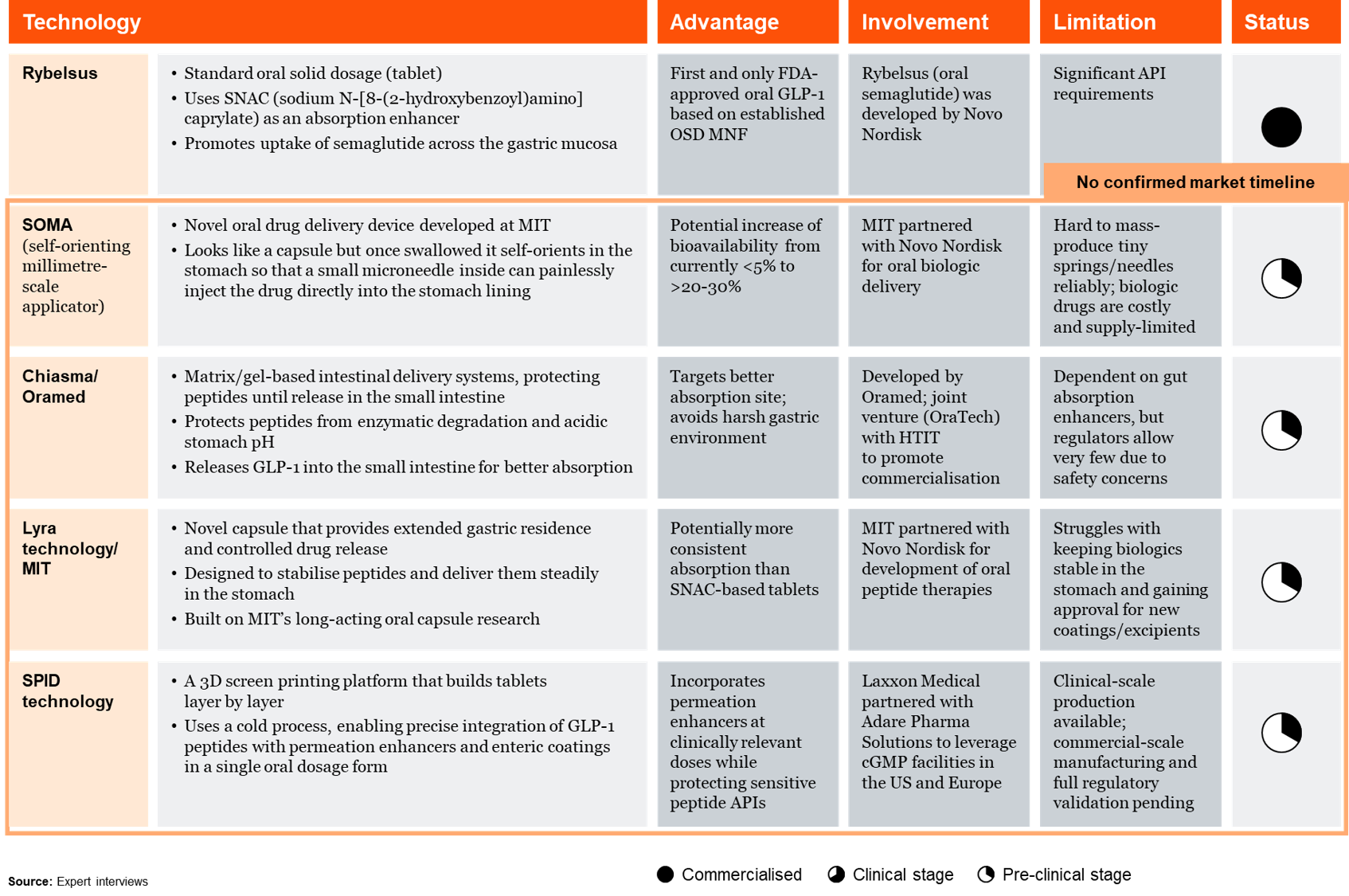
Several technologies are currently in development, with the aim of surmounting some of these challenges. However, most are still in their infancy. Each technology offers potential benefits like improved bioavailability or better absorption sites, but also faces challenges such as manufacturing difficulties, high costs, and regulatory hurdles.
Key OSD innovation in development
While oral GLP‑1s introduce greater upstream complexity and higher costs of goods, these realities are not always fully reflected in how oral therapies are perceived in the market. Experience with oral GLP‑1 use in diabetes has highlighted this disconnect: tablets are often not viewed as premium products, and the scientific and manufacturing innovation required to enable the oral delivery of biologics can be underappreciated – at times reduced to “just a pill.”
This perception gap may pose commercial challenges, especially when oral therapies are priced alongside injectable alternatives. Prescribers’ long‑standing preferences for established injectables, along with the commonly held view that injections are more effective, can also shape adoption. Still, these perceptions are not static and may shift as confidence in oral approaches grows.
While the opportunity for oral GLP-1s is substantial, realising its full potential will depend on how effectively pharmaceutical companies and CDMOs navigate the associated challenges.
How can Pharma and CDMOs overcome these challenges?
Translating oral GLP-1 innovation into scale places unprecedented demands on operational execution across the pharmaceutical value chain. Unlike traditional oral solid dosage products, oral GLP-1s require a distinct set of capabilities spanning advanced formulation and delivery science, specialised oral manufacturing for biologics, robust scale-up and lifecycle management, and resilient, high-quality supply chains. Meeting these demands goes beyond incremental upgrades to existing infrastructure and instead calls for purpose-built capabilities and closer coordination between pharmaceutical companies and CDMOs. As part of this, building robust direct-to-patient delivery models will be critical to ensuring timely, reliable access, supporting adherence, and reinforcing a differentiated patient experience. Together, these operational foundations are essential to reliably move oral GLP-1s from clinical promise to global commercial supply.
Scaling oral GLP-1s requires new manufacturing capabilities across the entire value chain
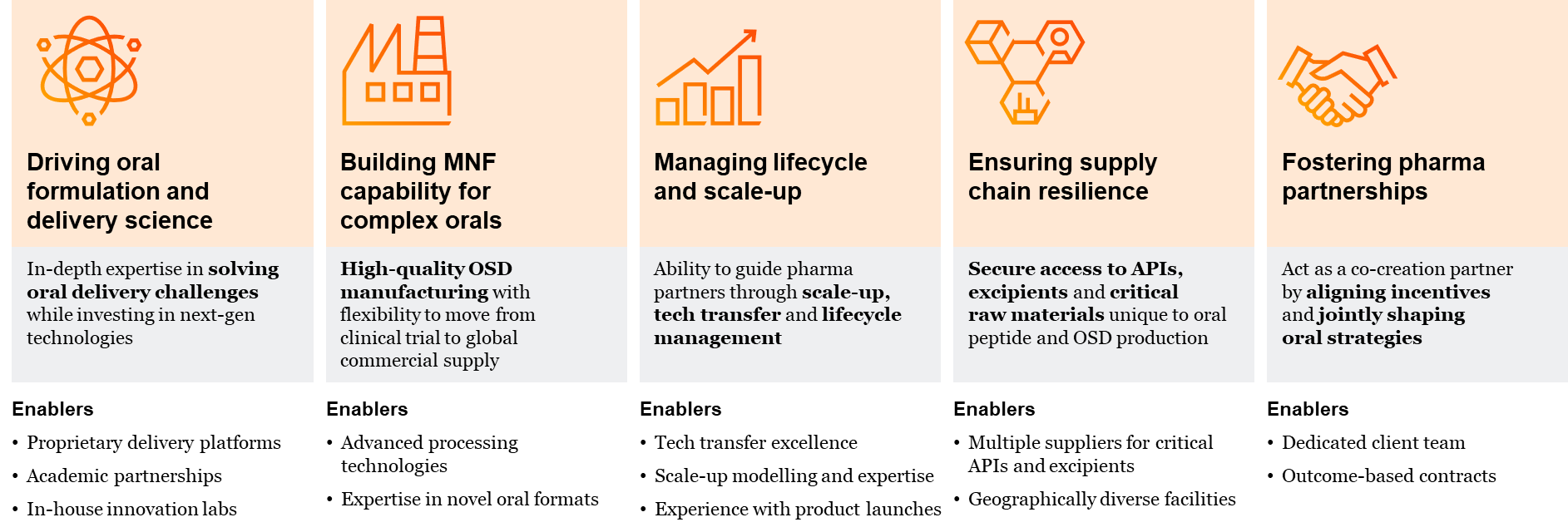
Note: MNF = Manufacturer
While operational excellence is essential to bringing oral GLP-1s to scale, commercial success will hinge on a distinct and equally demanding set of commercial and medical capabilities, with market education playing a pivotal role. Launching oral GLP-1s requires more than extending injectable playbooks; it demands the sustained education of prescribers, payers and patients on the clinical value, appropriate use and innovation behind the oral delivery of biologics. Companies must actively reshape ingrained perceptions that equate efficacy with injectables, while building confidence – particularly among general practitioners – who will be central to ensuring adoption on a broad scale. In parallel, education will be needed to support patients’ understanding, promote informed demand and reinforce long-term adherence in real-world use. Together, these capabilities form the demand-related basis required to realise oral GLP-1s’ full potential in the obesity treatment market.
Successful oral GLP-1 launches demand new commercial and medical capabilities
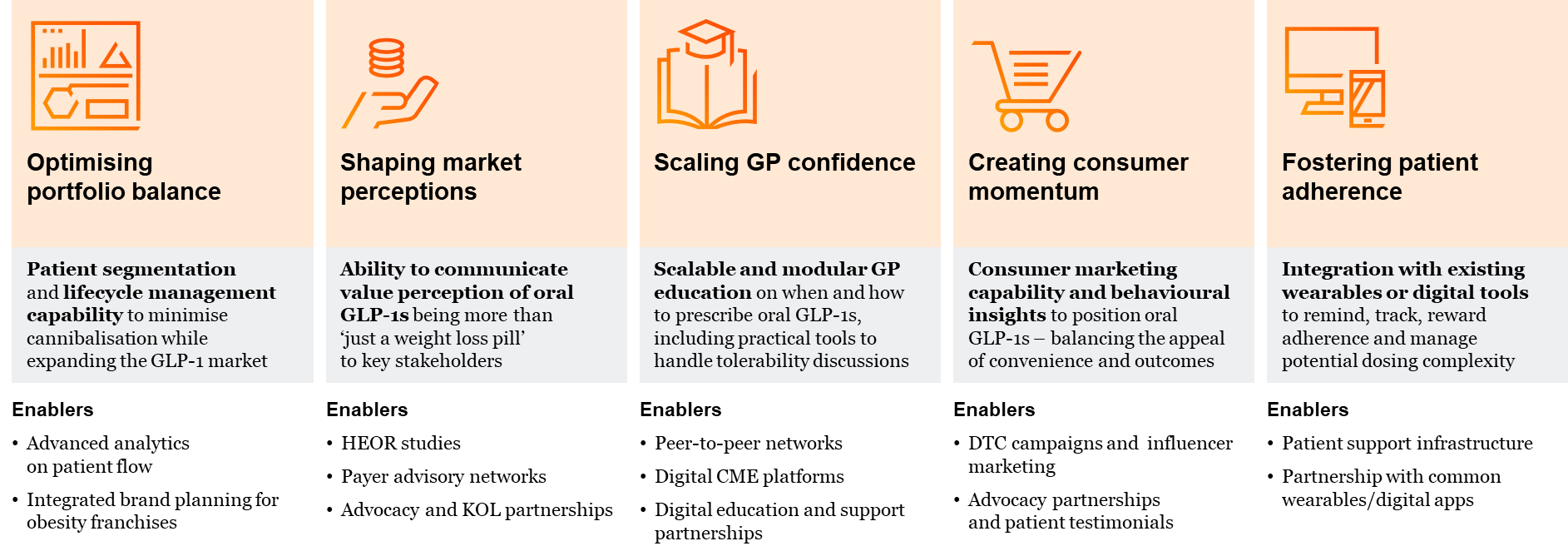
Note: DTC = Direct-to-consumer; GP = General Practitioner; HEOR = Health Economics and Outcomes Research; KOL = Key Opinion Leader
The time to act is now!
The window to shape the oral GLP‑1 market is open now—and it will not remain open for long. Decisions made today across manufacturing and commercialisation will determine which companies are best positioned as these therapies move from promise to scale. As the landscape evolves rapidly, early, deliberate investment in the right capabilities and strategic partnerships will be critical to securing a leadership position.
Contact us
Dr. Bodo Baumeister
Partner, Strategy& Germany
João Aguiar Machado